An absurd number of white-dominated institutions are “discovering” racism. Like every time white people are forced by media coverage of racist incidents to pay attention to racism, confronting the reality of systemic racism has made white people both individually and en masse quite uncomfortable.
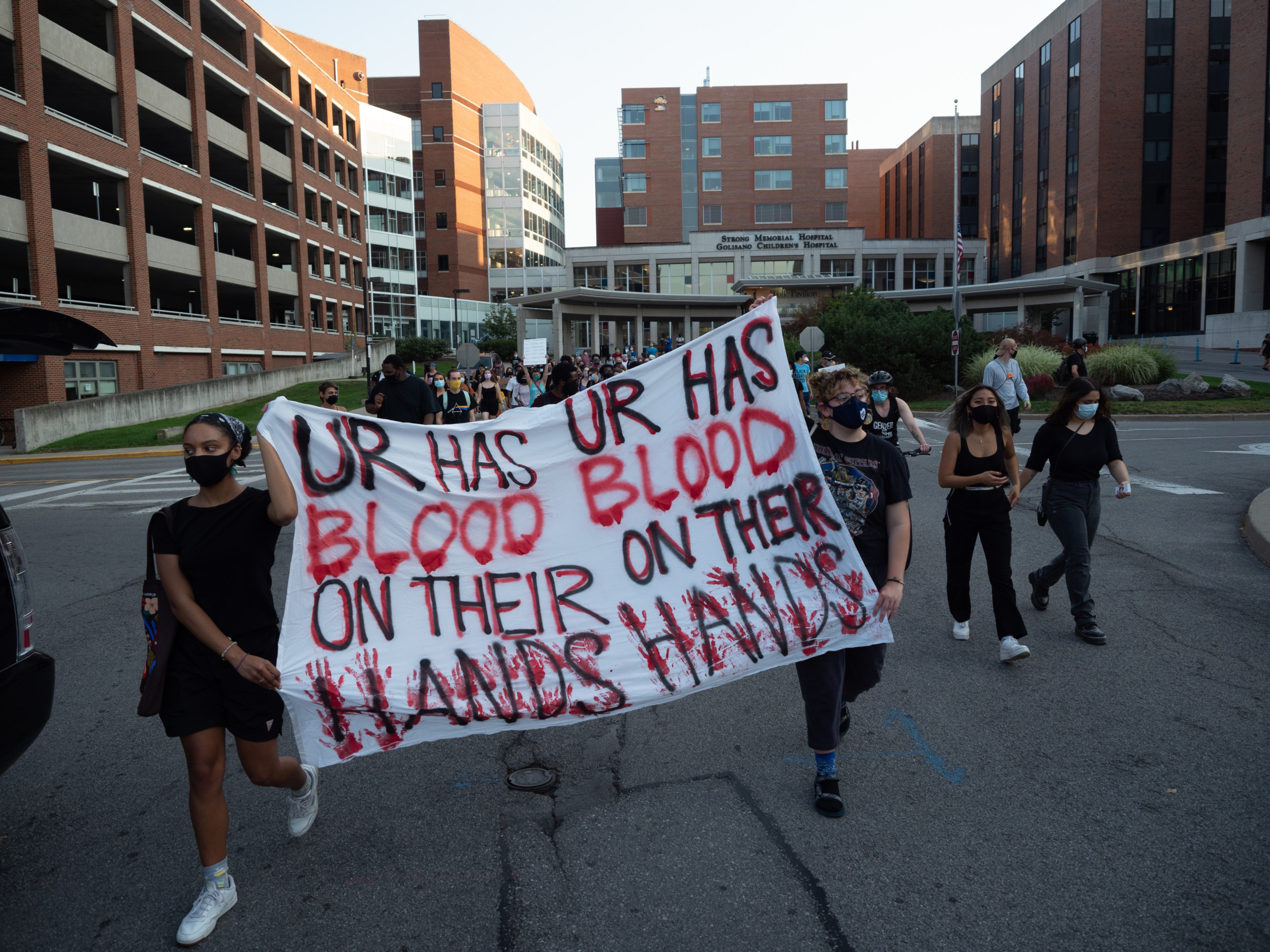
Now, institutions like UR are attempting to ease that discomfort with plans like the UR Medical Center’s Equity & Anti-Racism Action Plan.
I’m not interested in giving institutions props for finally waking up to the reality of systemic racism, but I’m especially bored by the notion that institutions should be patted on the back for targeting the most benign and uncontroversial goals possible.
Hire more people of color so that the staff actually matches the demographics of the surrounding neighborhoods? Wow, should have done that decades ago!
Collaborate with anti-racist community partners? Wow, you rebel, you! How cutting edge! How clever!
What an excellent use of University resources, to hire outside consultants and spend several months coming to the conclusion that, as it turns out, the demands that students of color nationwide have made for decades are, in fact, perfectly reasonable requests.
Nice job, guys. Thanks for finally metabolizing the obvious.
Now that I’ve covered the very bare bones efforts this plan makes, let’s tackle what it ignores.
Firstly, systemic racism is still alive and well in medicine, and it’s rooted in the development of medical science as a field. The “Father of Modern Gynecology,” for example, 19th-century doctor James Marion Sims, made his discoveries by experimentally operating on enslaved women without anesthesia.
Modern medicine is founded on substantial trauma for marginalized groups.
Eugenics experiments in California inspired Hitler’s medical experiments on live human beings. Following the 1927 Supreme Court decision Buck v. Bell, 70,000 people were sterilized in the U.S. after being deemed mentally ill, unintelligent, or otherwise undesirable additions to the gene pool. As recently as the period between 2006 and 2010, 150 female inmates were sterilized against their will in California — and doctors were paid just under $150,000 total to do it. Nurse Dawn Wooten’s recent accusations of forced and medically unnecessary hysterectomies at a Georgia ICE facility are the most recent evidence eugenics in medical science isn’t simply a relic of the past.
How can a medical facility as technologically advanced and prestigious as the University’s outright refuse to even name the reality of this practice? Do the creators of this plan simply lack the capacity to draw the connection between the historical past and deep mistrust in modern medicine today?
Finally, let’s consider the medical profession’s effects on women, which thanks to intersectional oppression has disproportionately impacted women of color. How about disgusting practices like the “husband stitch,” an extra stitch or two performed post-childbirth in order to sew up a woman’s vagina as tightly as possible for her husband’s pleasure? Let’s look at how many doctors nationwide perform medically unnecessary and dangerous C-sections, and are paid more for it.
Women are regularly discharged from hospitals while having heart attacks, because medical staff are trained to recognize the symptoms of heart attacks in men but not in women. Women are less likely to be taken seriously or treated for severe abdominal pain in emergency rooms. Meanwhile, chronic diseases like polycystic ovarian syndrome and pelvic inflammatory disease occur only in women, and have no treatment available on the market and no clear treatment plan — aside from urgent recriminations to “lose weight,” “exercise more,” and “lower stress levels,” because why not blame patients who are already suffering?
The medical industry could be instrumental in teaching the rest of society to acknowledge the statistical connection between sexual violence and women’s inflammatory diseases, eating disorders, and pain with sex. But the medical industry is less than invested in meeting women’s long-term needs.
This is just one quick survey of all of the many, many ways the medical system has failed and continues to fail the most vulnerable people forced to rely on it.
I fear that URMC has missed one of their best opportunities to come to terms with how they might be perpetuating these same problems in healthcare, and how their practices might be rooted — whether knowingly or not — in historic medical racism. Mitigating “barriers to access across the community” to “ensure equitable, accessible health care delivery” to Rochester’s disadvantaged citizens won’t mean anything if the care that marginalized people receive is rooted in well-documented medical biases and grounded in unacknowledged historical violence. Recent evidence has shown the connections between historical trauma, PTSD, and various medical problems.
Any approach to medicine that ignores this reality cannot begin to heal the same community ills that URMC acknowledges, but clearly doesn’t comprehend their own privileged role in upholding.